(some photographs, illustartions by courtesy of JAYPEE medical & SPRINGER publishers)
Paranasal sinuses are essentially air containing cavities lined by mucous membrane containing mucus glands as seen with the following illustration when a bright light is directed into the sinuses following functional endoscopic sinus surgery for this patient
As the nose and sinuses are intimately related to the orbit, skull base and thereby brain, it is of utmost importance to get a complete concept of this region in terms of surgical anatomy in order to prevent serious and life threatening complications of endoscopic sinus surgery.
Ideally understanding anatomy should begin with the following concepts:
Dry skeletal anatomy
Fresh Cadaver anatomy
Nasal endoscopic anatomy
Anatomy on the imaging scans
Anatomy during operating at times with the help of CT scans displayed in the operating theatre
The lateral wall of the nose is essentially composed of the following bones
Abbreviation used – SB- Skull Base, Mx – Maxilla, L- lacrimal bone, MT – Middle Turbinate, UP – Uncinate Process, ST – Superior Turbinate, Mx os – Maxillary sinus natural Os, SPA- Sphenopalatine artery entrance into the nasal cavity through SPF – Sphenopalatine foramen, IT – Inferior Turbinate, GL – Ground Lamella, B- Bulla ethmoidalis, LB – Lacrimal bone, PE – Posterior Ethmoid, NLD – Naso Lacrimal Duct, CP -Cribriform plate, LP – Lamina pyparacea, PEA – posterior ethmoid artery, ON – Optic Nerve, ICA – Internal Carotid Artery, FS – Frontal Sinus, FR – Frontal Recess, AN – Aggar Nasi, AEA – Anterior ethmoid artery, CG – Crista Galli, OlN – Olfactory Nerves, MMA – Middle Meatal Antrostomy, Dehi – Dehiscent, LLCP – Lateral Lamella of Cribriform Plate, ACF-Anterior Cranial Fossa, HS – Hiatus Semilunaris, PA – Pyriform aperture, MP – maxillary process, ANS – Anterior nasal Spine, S – Septum, CB – Concha Bullosa, PT – Paradoxical Turbinate, OMC – Ostio Meatal Complex, LW – Lateral Wall, SOF – Superior Orbital Fissure
Note -
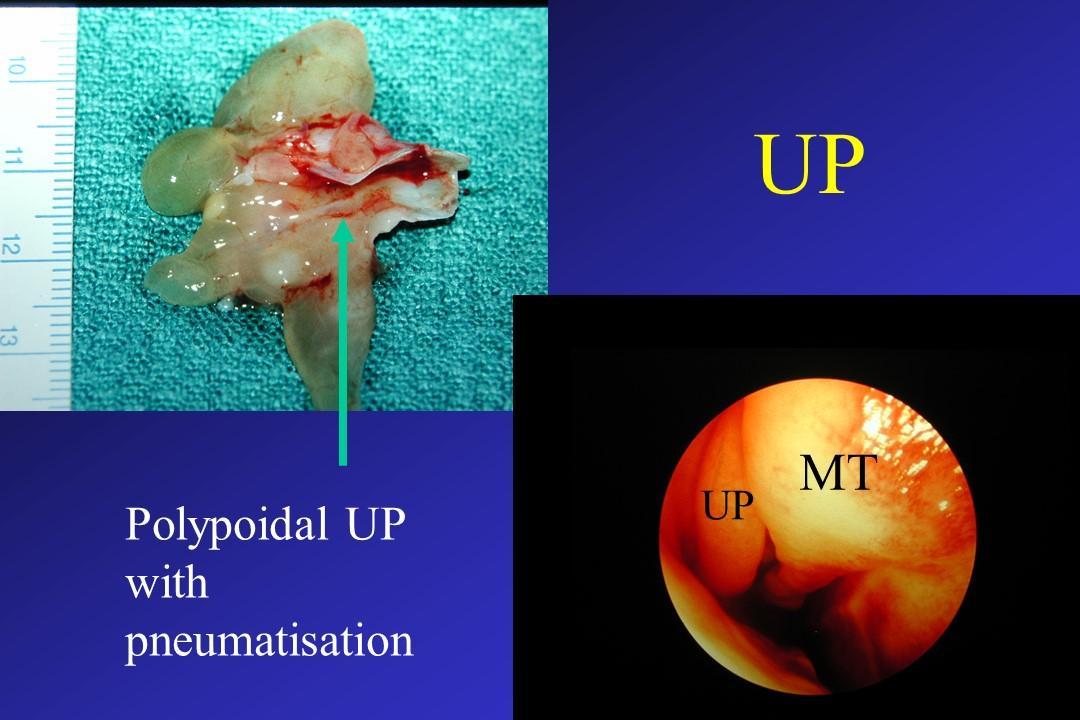
1) very thin skull base in the anterior part compared to the posterior part, the area of cribriform plate, forming roof of the ethmoid sinuses 2) the length of the middle turbinate with its upward extension as Ground lamella 3) position of the sphenopalatine foramen for the entry of the nerves and blood vessels ie, sphenopalatine artery, and sensory nerves coming out from the S.P ganglion, a site for the injection of local anaesthetic 4) the uncinate process in its lower one third goes posteriorly, the part that usually hides the natural os of the maxillary sinus 5) two small anterior and one posterior fontanelle divided by uncinate process covering these gaps” in the living subject
Further close up view of the lateral wall and the cadaver specimen to show uncinate process and bulla following displacing the middle turbinate
Note- variable anterior wall thickness of the sphenoid sinus wall- upper and lower part more thicker than the middle part, making easier for the surgeon to enter in to the sphenoid sinus if necessary through the middle part of the anterior wall. – LB- lachrymal bone, NLD- naso lachrymal duct
Ethmoid – THE most important bone
Maxilla
Sphenoid
Palatine
Many surgeons find ethmoid anatomy to be complicated in understanding but its not ! see the following schematic diagram Which shows a desk like structure with one drawer each side having 3 compartment Ie, anterior, middle and posterior. In the middle of the desk is a structure representing septum, with the upper projecting part as crista Galli, around which are multiple perforations as cribriform plate of the ethmoid also forming the anterior skull base.
The medial side of the desk has 3 elevations ie, lower, middle, and superior turbinate The posterior drawer representing posterior ethmoids, the middle one commonly known as Bulla (middle ethmoid), and the anterior one would be anterior ethmoids. The side of the desk would be the lamina pyparacia, the medial wall of the orbit.
When we articulate these bones will form lateral wall odf the nose as shown with various structures identified
Fronto ethmoid cavity in the right cadaver showing area of the frontal recess ,ant (AEA) and post( PEA) ethmoid artery, middle meatal antrostomy (MMA), lamina papyracia (LP)
Note- Right ethmoid cavity in cadaver. Note sphenoid is inferomedial to the posterior ethmoid and NOT a continuation of the posterior ethmoid !
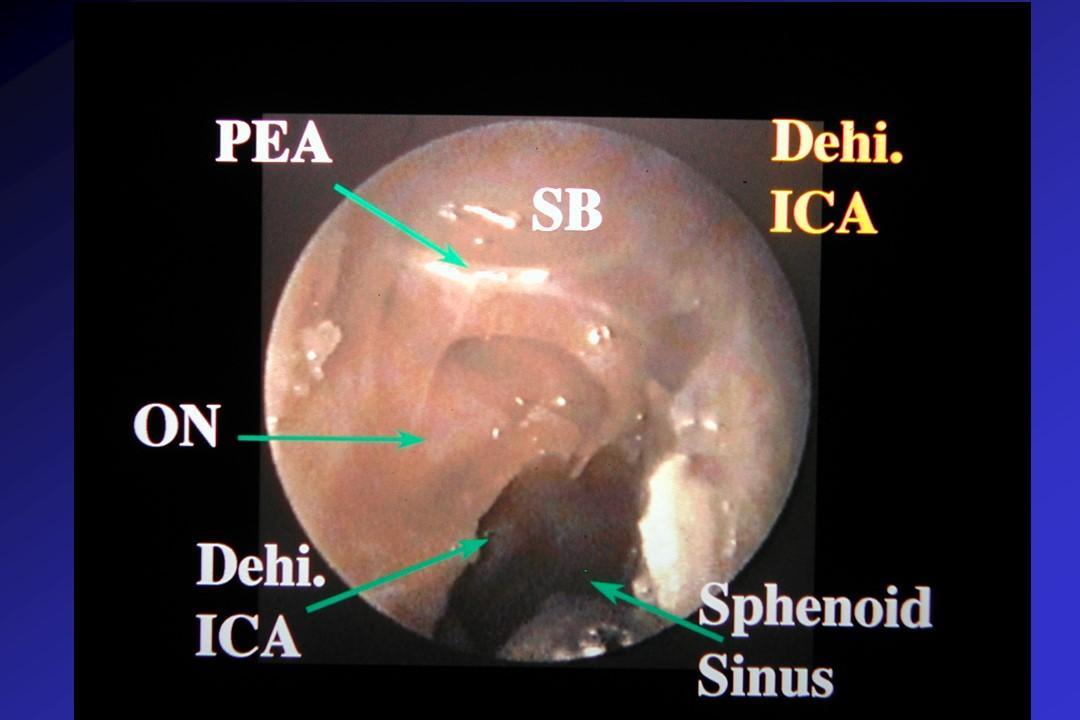
ON- optic nerve in post ethmoid, and the position of the sphenoid which is infero medial to the post ethmoid, dehiscent Internal carotid artery (ICA)
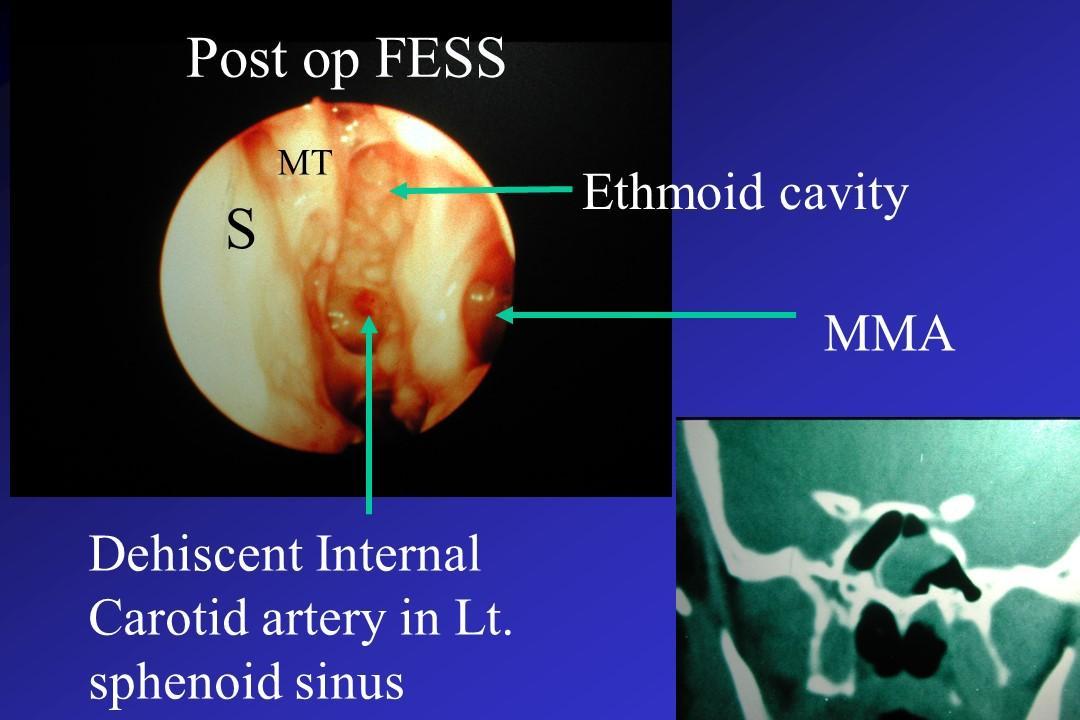
Close up view of the sphenoid with a dehiscent ICA
Sometimes in addition to the common anterior and posterior ethmoid artery, there is a middle ethmoid artery, and the surgeon should be aware of this
LLCP- lateral lamella of the cribriform plate.AN- Agger nasi cell, FS- frontal sinus, LP- lamina pyparacea, Note- frontal recess and Os is anterior to the ant. ethmoid artery AEA. View with a 70 degree ‘scope
ACF- anterior cranial fossa. Note- medial lamella of the cribriform plate is nine times thinner than the lateral part of the roof of the ethmoid which is formed by the orbital process of the frontal bone. It is the medial lamella of the ethmoid that is intimately related to the roof of the nose and during surgery this is the part more likely to be injured and result in CSF leak.
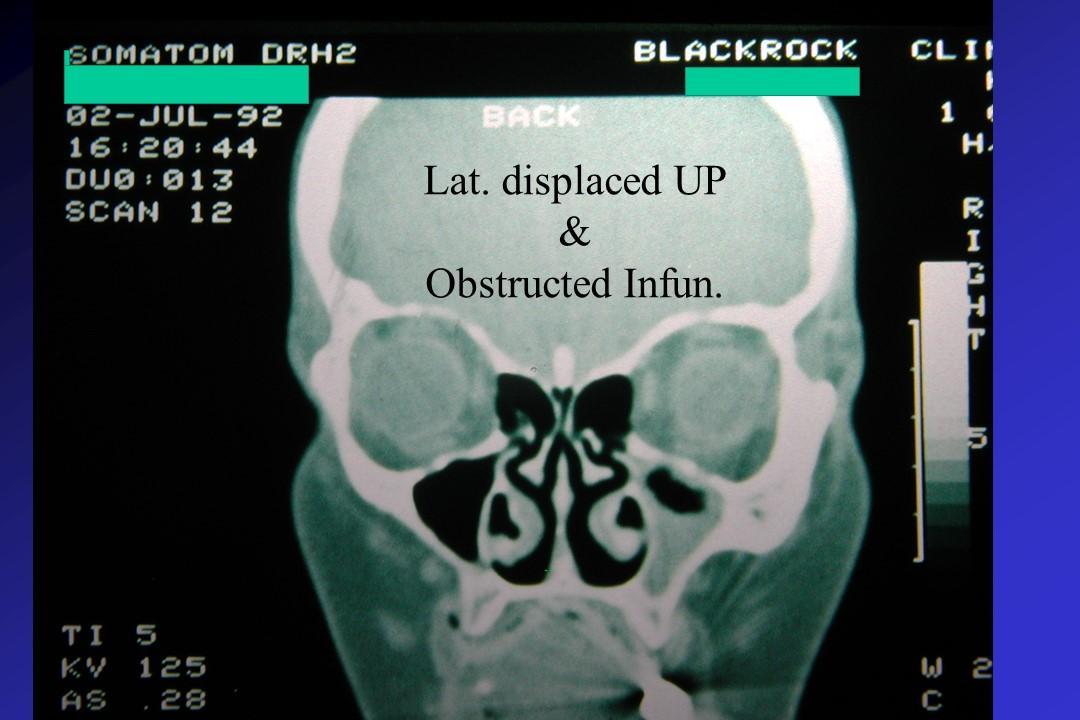
Note- cribriform plate and lateral lamella of the cribriform plate is lower than the fovea (roof) ethmoidales formed by the frontal . note – right uncinate process almost plastered on the lamina pyparacea, also note right hazy hypoplastic maxillary sinus.
Polypoidal bulla, active infection from ethmoids and maxillary sinus and polyp in the Middle meatus